


A nervous system expert explains why untreated clinician trauma can undermine patient care and how medical professionals can prepare more safely.
In a hurry? Here are the key points to know:
- Trauma training can activate unresolved, pre-verbal trauma in clinicians—often without conscious awareness.
- Patients co-regulate with clinicians; practitioner dysregulation can recreate traumatic dynamics.
- Burnout in trauma therapists is often a nervous system failure, not a motivation problem.
As trauma-informed care becomes central across medicine, psychology, and allied health, a difficult truth is gaining traction: The clinician’s own nervous system is not neutral in the treatment room. According to nervous system expert Irene Lyon, MSc, trauma therapists who have not done sufficient personal healing may unintentionally pass dysregulation on to the very patients they aim to help.
In a conference on why self-healing is not optional for trauma therapists, hosted by Conscious Life, Lyon challenged prevailing training models that prioritize techniques over lived nervous system regulation.
“The tools are good—we know they work,” she explained. “But the person, the vessel demonstrating and integrating them, that’s the piece that needs more attention.”
Drawing from somatic neuroscience, clinical training experience, and her own personal health collapse during trauma training, Lyon reframes self-healing as a core competency for trauma practitioners. For clinicians working with trauma, chronic illness, pain, or attachment injury, Lyon’s message is clear: Self-healing is not a personal luxury or wellness trend. It is a professional responsibility that directly affects clinical safety, attunement, and long-term practitioner health.
It is a professional responsibility that directly affects clinical safety, attunement, and long-term practitioner health.
Trauma Training, Activation, and the Clinician’s Nervous System
Lyon began by describing how trauma education itself can activate unresolved trauma in practitioners, particularly when the material involves violence, medical trauma, or early attachment injury.
“You’re going to be hearing about accidents, torture, rape, natural disaster, inescapable attack,” she said, noting that many trainees are not adequately prepared for how this material may affect their own bodies.
Crucially, this activation does not require conscious memory.
“Someone’s sitting there who didn’t know they had those things,” Lyon explained, “and all of a sudden they’re flashed back to the somatic experience of feeling like they’re being choked or trapped.”
This matters because the practitioner’s nervous system becomes part of the therapeutic field.
“If you have the inability to process your own sensations… your client is going to feel not well held,” she said.
Patients—especially those with early trauma—can perceive subtle shifts such as tension, shutdown, or emotional distance, often interpreting them as familiar relational threats.
Dissociation, Misattunement, and Ethical Readiness to Practice
One of Lyon’s strongest warnings concerned practitioner dissociation, what she described as “blacking out, not passing out, but going into daydream or dissociation.” In clinical work, this state creates what she calls a misattunement, where the patient senses the clinician’s absence even if nothing is verbally expressed.
“The worst thing… is a practitioner going into dissociation,” Lyon said. “And then the client is like, ‘What just happened?’”
Importantly, Lyon rejected the idea that clinicians must be fully “healed” to practice. Readiness, she explained, is about regulation, not perfection.
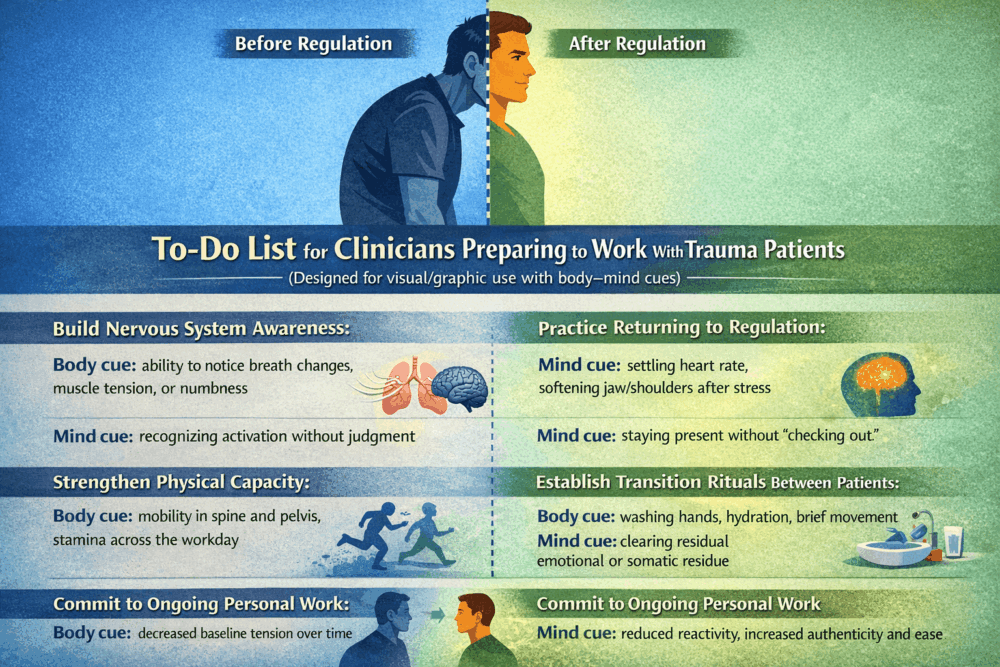
“A person is ready when they can hold their own physiology in highly stressful situations,” she said, and when they can return to regulation without relying on techniques mid-session.
Self-healing, in this context, becomes ongoing professional maintenance, essential for both ethical practice and clinician longevity.
Physical Health, Burnout, and Why This Matters for Medicine
Beyond emotional regulation, Lyon emphasized physical health as a neglected but essential factor in trauma work.
“Your self-care cannot just be meditation or nervous system work,” she said. “You need to walk, lift weights, move your spine.”
Without adequate physical capacity, clinicians may accumulate unresolved autonomic stress across sessions, contributing to burnout. Lyon reframed burnout not as a personal failure, but as a biological one:
“People burn out because they’re not in good regulation.”
This has profound implications for medical professionals. In trauma-informed care, the clinician’s nervous system actively shapes outcomes. Dysregulation can undermine trust, recreate attachment wounds, and shorten careers. As Lyon summarized:
“The tools work. It’s the person offering them that matters.”
For medicine and mental health alike, this represents a paradigm shift: clinician self-healing is not separate from patient care. It is foundational to it.






