


A trauma-informed, biopsychosocial reconceptualization of chronic pain and stress physiology for clinicians in medicine, surgery, psychiatry, rehabilitation, and trauma care.
In a hurry? Here are the key points to know:
- Threat physiology drives symptoms: What we call anxiety and chronic pain are hard-wired survival responses that manifest as systemic physiological changes, not just “psychological” phenomena.
- Adverse experiences shape lifelong biology: Early life stress can leave persistent inflammatory and threat responses that influence disease and trauma expression.
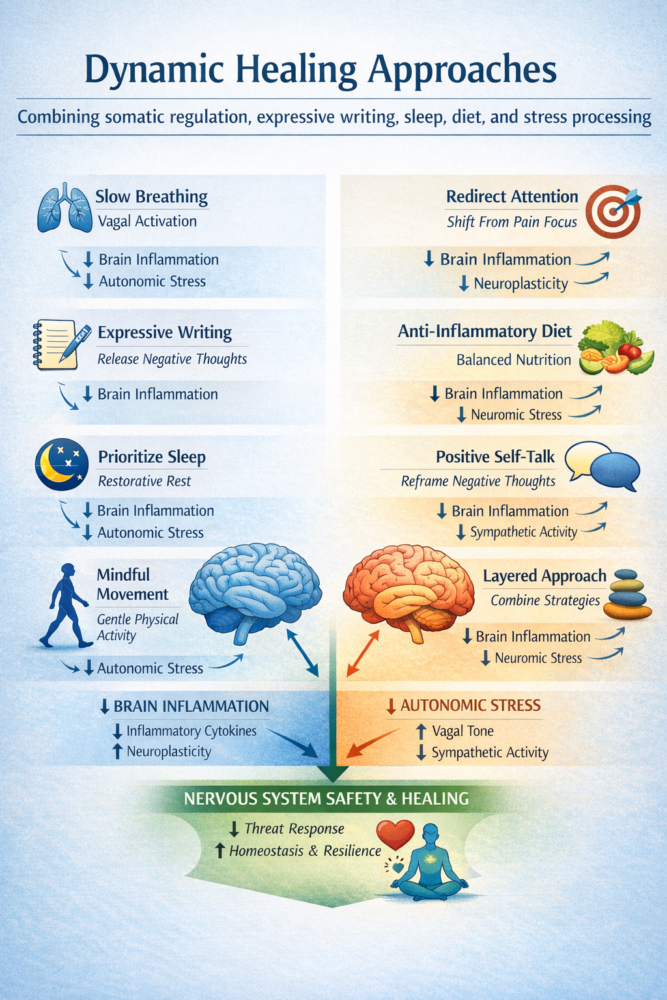
- Dynamic Healing approaches are integrative: Combining somatic regulation, expressive writing, sleep, diet, and stress processing can reduce chronic stress physiology and support healing.
At the 2023 Trauma Super Conference hosted by Conscious Life, spine surgeon turned chronic pain researcher Dr. David Hanscom presented a compelling case for reframing how medical professionals understand pain, stress, and trauma. Drawing from his own evolution from an orthopaedic surgeon treating failed back surgeries to an advocate for integrated pain resolution through his DOC Journey framework, Dr. Hanscom challenged conventional biomedical assumptions and offered a coherent, physiology-based narrative of trauma and healing.
Central to Dr. Hanscom’s message is the idea that “humans have a problem called consciousness,” which means that language and thoughts can trigger the same survival circuitry as physical threats. He stated plainly that “anything to do rationally to try to solve it [activated threat physiology] is impossible because… you can’t live without it.” This directly connects the experience of threat, whether physical or psychological, to physiological outputs that manifest as chronic pain, inflammatory responses, and disease states.
In repositioning chronic pain and stress as products of sustained threat physiology rather than isolated structural lesions or mere psychological constructs, Dr. Hanscom provides a framework that blends neurobiological insight with clinical pragmatism. For medical professionals — including surgeons, primary care physicians, psychiatrists, and rehabilitation specialists — this perspective invites a more integrated, neuro-immune view of trauma and patient care.
Consciousness, Threat, and Lifelong Stress Programming
Dr. Hanscom situates trauma and chronic pain within the context of human threat physiology. He explained that because language and thought are evolutionary novelties, they “create the same threat response as a physical threat” and engage fight-or-flight circuits that are “necessary… and incredibly powerful.” This reframes anxiety, a ubiquitous symptom observed across clinical settings, not as a psychological artifact but rather as a physiological state intrinsic to survival systems.
Hanscom also addressed how chronic exposure to threat states underpins many conditions often treated as separate clinical entities. He observed that chronic stress and activated threat physiology contribute to systemic inflammation, metabolic dysregulation, and immune shifts that extend far beyond pain alone, encompassing chronic diseases like hypertension, diabetes, and neurodegenerative disorders.
Critically, Hanscom highlighted Adverse Childhood Experiences (ACEs) as a biological imprinting mechanism, noting that individuals with high ACE scores can have elevated inflammatory markers decades later because they remain “programmed to look at life as dangerous.” This insight underscores how early life trauma creates a hyper-vigilant nervous system that predisposes patients to chronic threat physiology with implications for both pain practice and trauma-informed care.
Reframing Biomedical Assumptions and Therapeutic Integration
A cornerstone of Dr. Hanscom’s critique is the limitation of conventional biomedical models when confronting chronic pain and trauma. He underscores that most symptoms arise not from structural abnormalities but from physiological threat states: “90% of symptoms are physiological.” This observation supports growing evidence in pain science that structural findings on imaging often do not correlate with pain intensity and that nociplastic processes play a central role.
Rather than viewing talk therapy or rational interventions as curative, Hanscom champions what he calls “Dynamic Healing” — an integrative approach focusing on minimizing time in fight-or-flight physiology and maximizing cues of safety. Tools in this framework include somatic practices, breathing strategies (e.g., slow breathing to activate the vagus nerve), sleep optimization, diet adjustment, exercise, and expressive writing. Most notably, he stressed that expressive writing — having patients “write down your thoughts, throw them away” — has broad evidence of reducing inflammatory markers and facilitating healing.
Hanscom positions these interventions not as supplementary, but as central to addressing the neurophysiological processes that sustain chronic symptoms. He emphasized that these practices work not by suppressing negative states but by altering the nervous system’s response to threat, which, in turn, can reduce hyperreactivity and foster regenerative physiology.
A Clinically Relevant Paradigm Shift
The broader implication of Dr. Hanscom’s presentation is a call for a paradigm shift in clinical practice. By recognizing that chronic pain and trauma responses are anchored in activated threat physiology, clinicians can move beyond symptom management toward strategies that recalibrate the nervous system and support holistic healing.
This perspective elevates the importance of multidisciplinary and integrative care pathways, aligning medical, surgical, psychological, and rehabilitative interventions with the neurophysiological realities of chronic stress and trauma. It also reframes the clinician’s role: from seeking structural “pain generators” to facilitating patients’ mastery over their own physiological threat responses.
Ultimately, Dr. Hanscom’s synthesis reinforces that trauma and chronic pain are not isolated pathologies but manifestations of an ongoing survival response embedded in consciousness itself. Understanding this, clinicians across disciplines can embrace a more effective, evidence-aligned model of care — one that integrates threat regulation, systemic physiology, and patient empowerment to enhance healing.






