

Dr Pedram Shojai explains why trauma recovery often stalls—not in the mind, but in the body’s failure to register safety.
In a hurry? Here are the key points to know:
- Healing requires neuroceptive safety: If the nervous system remains in threat mode, sleep, immune regulation, and trauma processing are biologically inhibited.
- Bottom-up physiology matters: Gut permeability, inflammation, sleep disruption, and environmental stressors can perpetuate trauma symptoms despite effective psychotherapy.
- Safety is ecological, not singular: Sustainable recovery depends on aligning biological, relational, environmental, and behavioral factors—not on one intervention alone.
Despite advances in trauma-informed psychotherapy and pharmacology, a significant subset of patients fail to improve. Dr Pedram Shojai’s central thesis is that treatment resistance is often not psychological non-compliance, but physiological unsafety. Healing—whether psychological, immunological, or metabolic—requires a nervous system that has neuroceptively registered safety.
In a series of conferences on the impacts of trauma hosted by Conscious Life, Dr Pedram Shojai explained what supports cultivating nervous system safety. This information will benefit professionals working with trauma, the polyvagal theory, neuroception, and integrative clinical care.
Cultivating Nervous System Safety: What Trauma-Informed Clinicians Need to Know
A recurring challenge in trauma-informed care is the patient who understands their history, engages consistently in therapy, yet remains stuck—unable to sleep, regulate emotion, or experience sustained relief. In What Supports Cultivating Nervous System Safety, Dr Pedram Shojai argues that such cases are often misunderstood. The issue, he suggests, is not psychological resistance but physiological unsafety.
Shojai centers his framework on neuroception, a concept emerging from polyvagal theory that describes the nervous system’s unconscious assessment of safety or threat.
“Safety isn’t something that happens in the mind,” he explains. “Safety is something that happens in the body and in the nervous system.”
Even when patients cognitively recognize that danger has passed, their autonomic system may still be operating as if a threat is ongoing.
Crucially, Shojai highlights the vagus nerve and gut-immune interface as primary contributors to this ongoing alarm state. He notes that roughly 70% of immune tissue resides in the gut and emphasizes that microbial imbalance, gut barrier permeability, or food sensitivities can send continuous threat signals upstream.
“My body doesn’t speak English,” he says. “It speaks anxiety, it speaks insomnia, and it speaks in safety signals.”
From a clinical perspective, this reframes symptoms such as rumination, hypervigilance, and brain fog as expressions of immune and visceral signaling, not simply maladaptive thought patterns. Shojai points to cases where patients invest heavily in psychotherapy or even novel interventions while missing more proximal drivers.
“You’ve spent 30K going to ketamine clinics,” he notes pointedly, “but you still have a fire going on way closer to home than you thought.”
Sleep, in this framework, becomes a central diagnostic marker. Shojai describes sleep disturbance as a sentinel symptom of unresolved neuroceptive threat:
“The things that keep you from sleeping are the things that keep you from healing.”
Rather than viewing insomnia as a discrete disorder, he encourages clinicians to treat it as evidence that the nervous system does not yet perceive conditions as safe enough for restoration.
An Ecological Model of Safety and the Role of Agency
Rather than advocating for a single therapeutic solution, Shojai proposes what he calls an “ecology of resilience.” In this model, safety emerges only when multiple domains—biological, relational, environmental, and behavioral—are sufficiently aligned.
“It took all the king’s horses and all the king’s men to put Humpty Dumpty together again,” he says. “Do it all.”
Clinically, this challenges reductionist approaches that promise regulation through one modality alone. Shojai likens trauma recovery to gardening:
“It isn’t just planting the seed. It isn’t just watering it… It happens to be all of it.”
Patients may be eating well but sleeping poorly, or sleeping adequately while remaining in unsafe relationships or environments. Any single unresolved factor can undermine broader progress.
At the same time, Shojai underscores the importance of personal agency in nervous system regulation—while cautioning against interpreting this as blame. Modern healthcare, he argues, often reinforces passivity.
“People think they’re going to go to a place, have some service rendered to them, surgically extract their trauma, and go back to their life the next day,” he says. “That’s not how this works.”
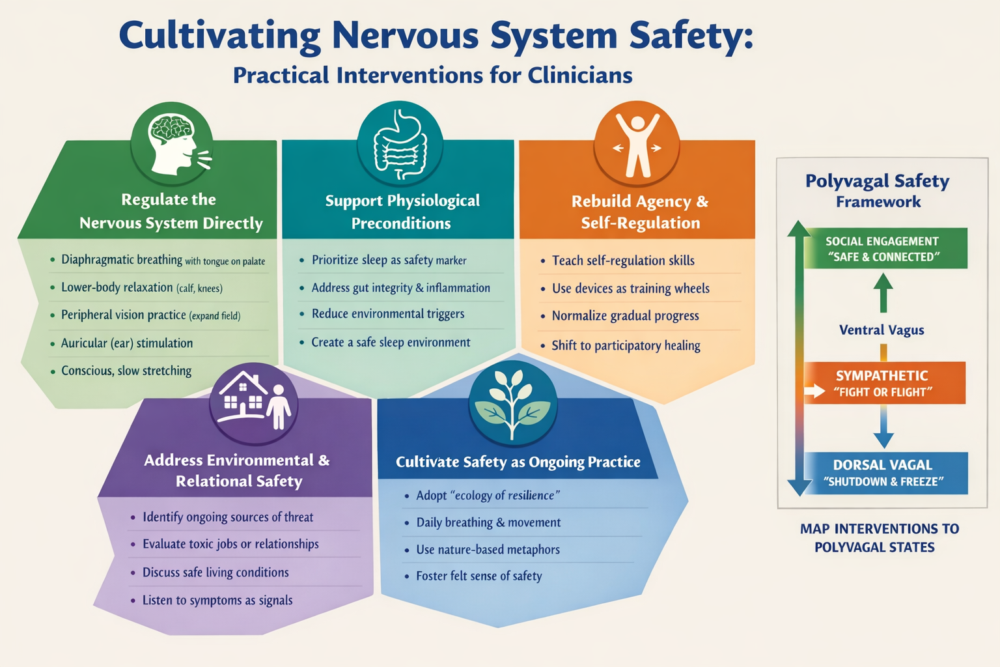
This emphasis on agency extends to practical interventions. Shojai outlines simple, low-cost practices that directly influence vagal tone and parasympathetic activation, including diaphragmatic breathing with tongue-to-palate placement, peripheral vision expansion, auricular stimulation, and conscious stretching. Importantly, he stresses consistency over novelty.
“You should be controlling your nervous system,” he says, “not asking other people to do it for you.”
For clinicians, this reframes patient “non-adherence” as a capacity issue rather than a motivational failure. Patients in chronic threat states may lack access to agency until their baseline physiological load is reduced—a process that often requires addressing sleep, inflammation, and environment first.
Clinical Implications and the Bottom Line for Clinicians
Shojai’s most clinically disruptive assertion may be his insistence that unsafety is often accurate. If a patient feels persistently unsafe, he argues, the appropriate question is not how to suppress that signal but what it is pointing toward.
“Where are the bears in your life?” he asks. “Is it your diet? Is it your environment? Is it your spouse?”
This perspective has significant implications for trauma-informed medical practice. It suggests that unresolved symptoms may reflect ongoing exposure to biological or relational threat rather than incomplete psychological processing. An unsafe home, chronic financial stress, inflammatory illness, or toxic relationship may continue to block healing regardless of therapeutic insight.
Shojai emphasizes the bedroom as a particularly critical environment.
“If you can’t feel safe in the place you lay your body down to rest,” he says, “you’re not going to feel safe anywhere.”
From sleep hygiene to environmental exposures, the conditions required for restorative shutdown must be actively cultivated.
For clinicians, the challenge is twofold: to validate symptoms as meaningful signals while helping patients methodically reduce the sources of threat those signals reveal. This often requires interdisciplinary collaboration and a willingness to address lifestyle and environmental factors alongside conventional treatment.
Bottom line for clinicians: Trauma recovery stalls not because patients lack understanding, but because their nervous systems remain unconvinced that danger has passed. Healing becomes possible when care extends beyond cognition to include physiology, environment, relationships, and agency—allowing the body, finally, to register safety.






